This article explains the term diffuse disc bulge commonly found on the reports of magnetic resonance (MR) and computed tomography (CT) images of the spine.
What is the spinal disc?
The spinal or intervertebral discs are cartilages between the bones (vertebra) in the spine (Picture 1).
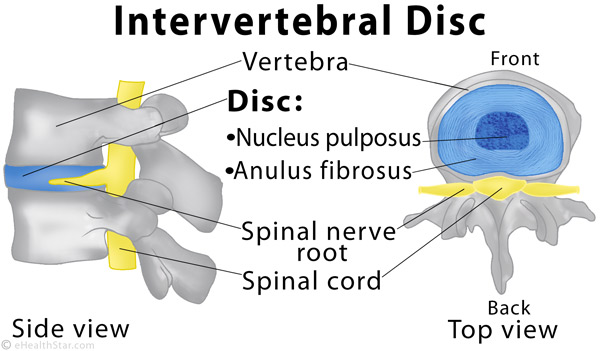
Picture 1. A normal spinal or intervertebral disc
What is a disc bulge?
A disc bulge is a condition in which at least 25% (90°) of the disc’s circumference extends beyond its normal limits and the soft disc center does not break out through the outer fibrous ring (Picture 2) [1].
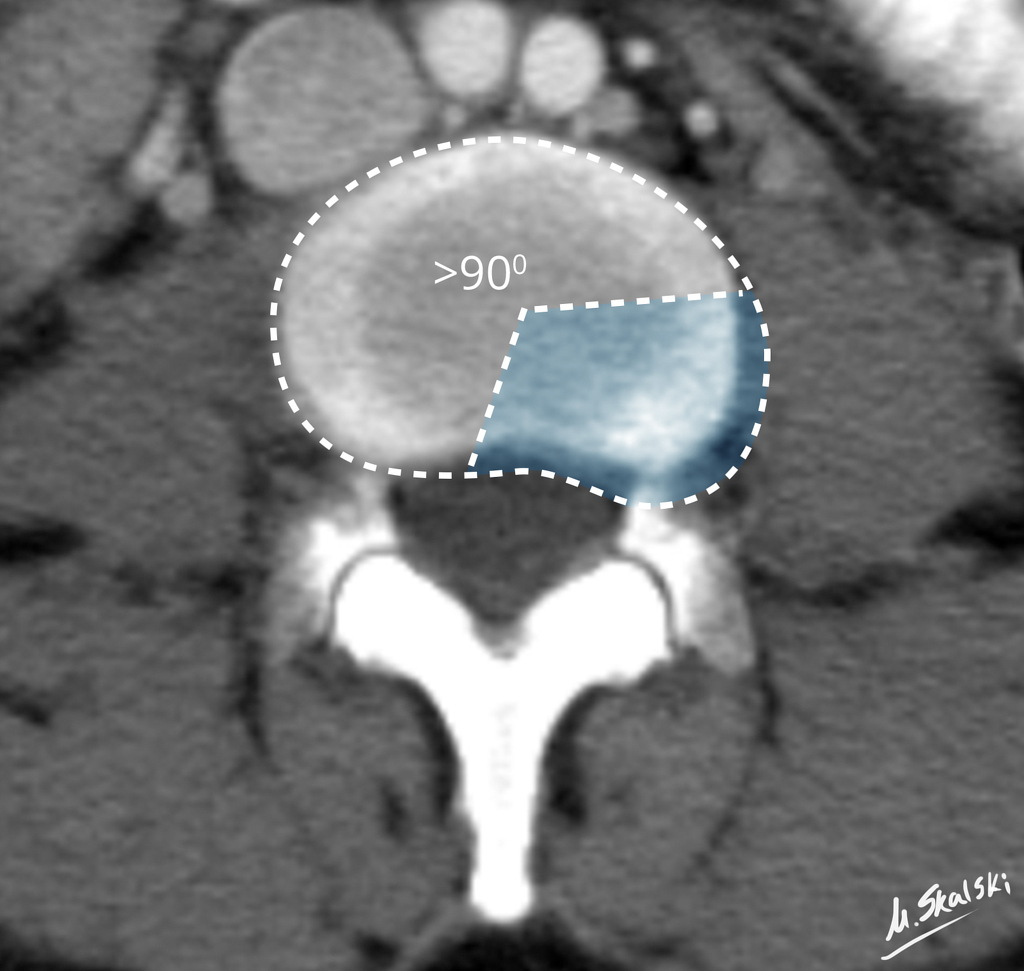
Picture 2. A CT image of a disc bulge (blue) (source: Radiopaedia, CC license)
What is a diffuse disc bulge?
The term diffuse disc bulge has no specific meaning but just describes a disc bulge in general. However, some doctors may use it instead of a broad-based herniation.
A disc bulge rarely causes any symptoms while a disc herniation can put pressure on the spinal nerve roots and cause pain in the neck, back, arm or leg. If your magnetic resonance (MR) or computed tomography (CT) image report mentions a diffuse disc bulge and it is not clear what it means, ask your doctor.
Details about the causes, symptoms, treatment and prevention of a bulging and herniated disc.
What is a diffuse annular bulge?
A diffuse annular disc bulge is just a long term for a disc bulge but some doctors use it when they want to emphasize that only the outer part of the disc called annulus fibrosus is involved in the bulge and there is no herniation.
What is a minimal or mild diffuse disc bulge?
In a minimal or mild disc bulge, the disc extends only slightly beyond its normal limits and rarely causes any problems.
What is a circumferential diffuse disc bulge?
A circumferential diffuse disc bulge extends over 50-100% of the disc’s circumference [1]. Note, that the severity of the symptoms tends to decrease with the percent of the disc’s circumference involved.
What is a posterior and posterolateral diffuse disc bulge?
A posterior or central diffuse disc bulge points backward to the spinal cord [1].
A posterolateral diffuse disc bulge points backward and laterally to the right or left spinal nerve root and may cause pain in an arm or leg.
What does the diffuse disc bulge L4-L5 or L5-S1 mean?
- The disc L4-L5 is the one between the 4th and 5th lumbar vertebra in the lower back.
- The disc L5-S1 is the one between the 5th lumbar and 1st sacral vertebra in the lower back.
If one of these discs bulges out, it may, rarely, cause pain in the lower back, buttock or leg.
- References
- Fardon DF et al, 2014, Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology The Spine Journal
My MRI Result shows:
Mild Moderate Discovertbral degenerative changes evidenced with
* Multilevel dessication (pfirrmann II/III) with small anterior marginal osteophytic growth
* Multilevel diffuse disk bulge with LI-L2 moderate spinal canal stenosis, L2-L3 mild spinal canal stenosis, L3-L4 & L4-L5 lateral recess stenosis,
* L2-L3 & L3-L4 Horizontal anular fissure
Hello can you help me understand my MRI results please
Mild disc and facet degenerative change predominantly at L5-S1..
There is no evidence of canal or foraminal stenosis.
Narrative
EXAM: MRI LUMB SPINE WO CONT
Clinical history: Lumbar radiculopathy
INDICATION: . Other low back pain
COMPARISON: None
TECHNIQUE: MR imaging of the lumbar spine was performed using the following
sequences: sagittal T1, T2, STIR; axial T1, T2.
CONTRAST: None.
FINDINGS:
There is normal alignment of the lumbar spine. Vertebral body heights are
maintained. Marrow signal is normal.
The conus medullaris terminates at L1. Signal and caliber of the distal spinal
cord are within normal limits.
The paraspinal soft tissues are within normal limits.
Lower thoracic spine: No herniation or stenosis.
L1-L2: No herniation or stenosis.
L2-L3: No herniation or stenosis.
L3-L4: No herniation or stenosis.
L4-L5: No herniation or stenosis.
L5-S1: Disc desiccation and loss of disc height. Mild facet arthropathy. Mild
central disc protrusion with annular fissure. Canal is patent. The foramina are
patent
Also the pain im feeling I didn’t start having until i had an car accident in February 2022. This pain is so unbearable it shoots up my back and down my legs. One day I heard a pop while carrying a bag of cereal. My doctor’s main suggestion was to lose weight. When my weight didn’t cause my pain
I had similar conditions after car accident as well that MRI shows C6/7 herniation and T10/11 herniation. Pains could be bad but it seems it’s very confusing what is happening that doctors would refer it to aging even it’s after only after accident
I’m in desperate need of some help….I’ve had 2 back surgeries, both 2018, but now in 2022 I’m back here in the worst pain I’ve thought imaginable. The pain in my back, hip, knee, foot, and as of 3 days ago, my testicles, if absolutely unreal. I’m on chronic pain therapy for this; and the narcotics don’t even touch the pain, I’m talking from a 10 to 9.99, and that’s on morphine & hydromorphone. On top of this, I am developing extremely, mind numbingingly painful kidney stones. They won’t operate on me because of my age (32) and I’m suffering every second of the day. Is there any service that can advocate for me before I kill myself? I’m at the point of taking my own life the last 8 weeks have been so difficult….
Thomas,
I hope you got some help. Your post was heartbreaking….
I’ve had sciatica since 2014. And since my vaccine now everything is worse including my neck.
Again, I hope you got help
Susie |
I too suffer severe pains in my vaginal area’ I be had many MRI, CT even Ultra sounds. I suffer pain & you’re right there is no pain medicine to help except I do fine coincidently the medication. Baclofen helps for at least a while. Try stretching twice a day. The pain will subside a little bit. Try a diet of low alkaline. Don’t eat in the morning because the food carries weight. Stay off your feet as much as possible.
Hello, I am having severe lower back pain which radiates along my hip, groin, and down my leg to my foot. Can you help me decipher these MRI results from last week:
Lumbar spine MRI with and without contrast
CLINICAL HISTORY:
Lumbar spine pain continues even after surgery about 1 year ago
TECHNIQUE:
Multiplanar multisequence MR imaging of the lumbar spine was performed before
and following the intravenous administration of contrast.
Prohance 20ml
FINDINGS:
For the purposes of this exam, the last well-formed disc space will be labeled
L5-S1.
Stable postsurgical changes of right hemilaminectomy at L5-S1. Straightening of
lumbar lordosis, likely related patient positioning or muscle spasm. Trace grade
1 retrolisthesis of L3 on L4. Remaining lumbar vertebral bodies are in
satisfactory alignment. Vertebral body heights are normal. There is no
suspicious focal bone marrow lesion. There is no bone marrow edema to suggest
fracture. The conus terminates at L1-L2 disc space.
Disc desiccation and disc space narrowing, which is greatest in the lower lumbar
spine at L3-L4 and L5-S1. Significant endplate signal degenerative changes at
the right aspect of L4-5. This is seen to a lesser degree at L3-L4. Multilevel
facet arthropathy. Slight dextrocurvature of the lumbar spine with the apex at
L3.
Level specific observations, as follows:
T12-L1: Mild diffuse disc bulge. No significant spinal canal stenosis or
foraminal narrowing.
L1-2: Mild bilateral facet arthropathy. Minimal diffuse disc bulge. No
significant spinal canal stenosis or foraminal narrowing.
L2-3: Mild bilateral facet arthropathy. Mild diffuse disc bulge. No significant
spinal canal stenosis or foraminal narrowing
L3-4: Moderate bilateral facet arthropathy. Disc protrusion diffusely at L3-L4.
No significant spinal canal stenosis. Mild inferior right foraminal narrowing.
L4-5: Moderate bilateral facet arthropathy. Diffuse disc protrusion with right
paracentral inferior disc extrusion resulting in right lateral recess stenosis
with abutment of the descending L5 nerve root. At least moderate right foraminal
narrowing. Mild left foraminal narrowing. No significant spinal canal stenosis.
L5-S1: Moderate bilateral facet arthropathy. Diffuse disc bulge with far lateral
disc protrusions. No significant spinal canal stenosis. Moderate right and mild
left foraminal narrowing.
Enhancement in the soft tissues posterior to L4-5, likely related to prior
intervention/partial discectomy. No well-defined fluid collection. Partially
imaged adnexal cysts on a single T1 sequence measuring 7.3 cm on the right and
5.3 cm on the left, similar to prior CT from 11/20/2018.
IMPRESSION:
1. Postsurgical changes of right hemilaminectomy at L5, unchanged. Tract of
enhancement in the posterior subcutaneous soft tissues leading to the L4-5
interspace, likely related to prior intervention/partial discectomy.
2. Right paracentral inferior disc extrusion at L4-5 resulting in right lateral
recess stenosis and abutment of the descending L5 nerve root. At least moderate
right and mild left foraminal narrowing at this level.
3. Multilevel disc bulges with at least moderate right/mild left L5-S1, and mild
inferior right L3-L4 foraminal narrowing. No areas of significant spinal canal
stenosis.
4. No abnormal dural enhancement or fluid collections identified.
Thank you!
WHAT DOES ALL THIS MEAN?
1. at L3/L4 to have fluid in the facet joints and a circumferential disc bulge measuring 2.5 mm producing effacement of the thecal sac and mild bilateral neural foramen stenosis.
2. at L4/L5 there is mild bilateral facet arthropathy, fluid in the facet joints and a circumferential disc bulge measuring 4mm producing mild ventral canal stenosis and moderate bilateral neural foramen stenosis touching the bilateral L4 nerve roots?
3. at L5/S1 level there is mild bilateral facet arthropathy, fluid in the facet joints and a circumferential disc bulge measuring 3.5mm producing central canal stenosis and moderate bilateral neural foraminal stenosis touching bilateral L5 nerve roots?
4. AND abnormal straightening of the normal lumbar curvature suggesting muscle spasm?
Hi if you can please help me out to figure out my MRI test results it came back as 1mm broad-based central disc bulge at the L5-S1 level. there is 1mm of diffuse broad-based bulging at the L2-L3 level, the reason i need your profession help to understand if i have a disc problem because of all my symptom I’m going through i know for sure i hade a hip problem but of course just because Im young Orthopedic don’t want to deal with my situation can you please help me out to figure out if i have a disc problem from this result I got
Hi, kindly interpret my MRI.
There is preservation of lumbar lordosis. There is no loss of vertebral body height no evidence of a suspicious bone marrow signal abnormality. Conos is normal in caliber position and signal. Survey paraspinal soft tissues remarkable. There is multilevel loss of disc hydraton and bulge, there is bilateral facet and ligamentum flavum hyperttophy becoming more pronounced inferiorly.
LI-2 through L3-4 disc bulge without focal disc herniation, significant central canal or neural foraminal stenosis.
L4-5 disc bulge, facet and ligamentum flavum hypertrophy cause moderate central stenosis. No focal herniation. Bulge and facet hypertrophy cause mild bilateral foraminal stenosis.
L5-S1 disc bulge with superimposed broad based posterior disc
herniation causing central canal stenosis. Bulge and facet hypertrophy
caused mild bilateral foraminal stenosis.
I go to a physical therapist twice a week, should I also see a chiropractor? Can use of an inversion table help with the healing, Please advise. Thank you very much.
Sir,
I had accident in May of 2018. Since then I’ve been having pain and grinding in Neck. Upper back pain and Arm and shoulder pain. I also get leg, buttock pain and burning.
Extensive MRIs have been done (Cervical, Thoracic and Lumbar). once in August of 2018 and then again in February of 2019. Have also had EMG and EEG tests (no issues). And Rheumatologists ran tests for autoimmune (no issues). Neurosurgeons are saying surgery is not needed and after 6 months of Physical therapy, my symptoms are still there.
I am now considering PRP (prolotherapy) but would appreciate your guidance/take on this.
Notes (that had issues) from my Cervical MRI
=====================
C3-C4: Small tiny central disc osteophyte complex. Minimal effacement of ventral thecal sac. Neural foramina
are intact. Facet joints are unremarkable. Thecal sac: 1.0 cm AP.
C4-C5: Posterior osteophyte C4-5 noted. Circumferential broad-based bulging disc seen. Effacement ventral
thecal sac and cord noted. Narrowing of the neural foramina, greater on the right than the left. Facet joints are
unremarkable. Thecal sac: 0.9 cm AP.
Notes (that had issues) from Thoraci MRI
=====================
T8-T9 demonstrates a mild left paracentral protruded disc with minimal effacement of ventral thecal sac.
Minimal, if any, neural foraminal encroachment noted. Cord is intact.
T9-T10 tiny central protruded disc identified. This causes effacement ventral thecal sac and abuts the cord.
Neural foramina are intact.
(no issues in Lumbar MRI).
Thank you in advance.
* Straightening of Lumbar spine likely due to paraspinal muscle spasm.
* Disc Dessication noted in all lumbar intervertebral disc.
* Schmorl’s node seen at end plates of L1, L2, L3 vertebra.
* L1-L2, L2-L3 are normal.
* while in L3-L4: Disc space is normal, DIFFUSE POSTERIOR and LEFT EXTRAFORAMINAL DISC BULGE COMPRESSING THE LEFT Traversing Nerve Roots.
* IN L4-L5: Disc space is normal but Diffuse posterior disc bulge causing Identification of Anterior Thecal sac, Narrowing of bilateral neural foramina and compression effect over bilateral existing and traversing nerve roots.
* L5-S1 are normal.
please suggest me the actual problem
Sir From few days ago i am feeling burning pain in my left lower spine and but thats my mri report kindly suggest me
At L1-2 level, disc shows preserved margin. No significant foraminal stenosis or exiting nerve root
compression is seen. Spinal canal is ample at this level.
At L2-3 level, disc shows preserved margin. No significant foraminal stenosis or exiting nerve root
compression is seen. Spinal canal is ample at this level.
At L3-4 level, disc shows preserved margin. No significant foraminal stenosis or exiting nerve root
compression is seen. Spinal canal is ample at this level.
At L4-5 level, subtle circumferential disc bulge is noted with subtle encroachment in lower third
of both neural foramina. Spinal canal is ample at this level.
At L5-S1 level, posterior annulus fibrosis fissure is seen with subtle posterior disc bulge causing
ventral thecal sac compression. No significant neural foraminal stenosis is seen. Spinal canal is
ample at this level.
Please help me understand these MRI with die contrast results.
My symptoms are extreme low back pain moving down my right buttocks and leg, numb toes, sharp pain in my low back, aching and burning pain in my mid back, loss of bladder control and bowel control
Normal alignment of the lumbar spine is seen. No bone marrow edema, fracture or subluxation isnoted. Spinal cord demonstrates normal size and normal signal. Conus medullaris terminates at theL1-2 level. No enhancing lesions are seen in the spinal cord.
At L1-2, no significant disc bulge or protrusion is seen. No spinal canal or foraminal narrowing isnoted. Facet arthropathy is noted bilaterally.
At L2-3, no significant disc bulge or protrusion is seen. No spinal canal or foraminal narrowing isnoted. Bilateral facet arthropathy is seen.
At L3-4, no significant disc bulge or protrusion is seen. No spinal canal or foraminal narrowing isnoted. Bilateral facet arthropathy is noted.
At L4-5, 1 mm disc bulge is asymmetric to the right. Facet arthropathy is noted bilaterally. Mild rightforaminal narrowing is noted without left foraminal narrowing. No spinal canal narrowing is noted.
At L5-S1, 1 mm central disc protrusion is seen. Bilateral facet arthropathy is noted. No significantspinal canal narrowing is seen. Mild bilateral foraminal narrowing is noted.
IMPRESSION:1. Mild spondylosis is seen with foraminal narrowing appearing mild on the right at L4-5 andbilaterally at L5-S1 but no significant spinal canal narrowing is seen. Multilevel facet arthropathy is noted.
Oh I forgot to note that all symptoms started after a bad fall. I also have laws of motion in my toes And have loss of balance. Symptoms are better or worse throughout the day depending on activity. 🙁
Posterior annular tear at l4l5. Diffuse disk bulge at l4l5. Mild disk bulge at l5s1 and moderate spinal canal stenosis. Lumbar spasms.
My mother is suffering from tremendous back pain . Dector said only surgery is the options after seeing the MRI report.
Could your please help me what should I do.
MRI findings:
Clinical History: Back pain.
FINDINGS:
Lumbar lordosis is partly straightened.
Vertebral bodies are normal in height, alignment and marrow signal intensity. Posterior spinal elements are normal.
Significant advanced spondylotic changes are seen in the visualized vertebrae as evidenced by
marginal osteophytes, disc desiccation and Schmorl’s node formation at multiple levels.
L1-L2 : Disc desiccation along with reduced disc height and mild posterior disc bulge is seen
narrowing the bilateral lateral recesses leading to compression on bilateral descending nerve
roots. AP canal diameter is 10 mm. Bilateral neural foramina are normal in caliber.
L2-L3 : Disc desiccation along with diffuse circumferential disc bulge is seen indenting the anterior
thecal sac (with secondary spinal canal stenosis) and markedly obliterating bilateral lateral
recesses leading to compression on bilateral descending nerve roots. AP canal diameter is 7 mm.
Bilateral neural foramina are normal in caliber.
L3-L4 : Disc desiccation along with diffuse circumferential disc bulge and small posterior central
disc protrusion is seen markedly indenting the anterior thecal sac (with significant secondary
spinal canal stenosis) and markedly obliterating bilateral lateral recesses as well as neural
foramina leading to compression on bilateral descending & exiting nerve roots. AP canal diameter
is 4 mm.
L4-L5 : Disc desiccation along with diffuse circumferential disc bulge and small posterior central
Hi there.
Looking for some advice on MRI and X-RAY results.
I was diagnosed via x-ray with missing T12, and a transitional L6 (one sided)
Further too physio therapy, acupuncture, cbt, medication I was given an MRI. The results I was given were that I have L3:L4 diffuse disc bulge encroaching into right foramina abutting nerve exit root.
L4/5: disc desiccation and diffuse disc bulge, encroaching into both neural foramina abutting never exit root bilaterally.
All other discs are unremarkable.
Since had 8 facet injections. The radiologist explained that the L6 transitional is causing a curve in my spine.
Possibly early forminal stenosis.
I am concerned as my MRI results don’t mention anything about a curve or stenosis. Although he pointed things out to me.
I am due to see consultant this month and would really appreciate a better understanding of the MRI results. So I don’t go in there clueless.
Seem painkillers are the ‘in’ thing at the moment. Doctors doubled my pills yday. After an horrendous day this week that see me not walking without almost screaming in agony.
Things have got worse in the last 8 months and I think the consultant will not re scan to investigate.
Also, have you any information on how a transitional vertebrae causing disc problems is treated? Is a desiccated disc a sign of degenerative disc disease and there is more to come in figure due to the curve etc.
Thank you very much.
Krystal
L4-5 diffuse disc bulge with concentric posterior annular tear indenting anterior theca causing mild bilateral neural foraminal compromise.
Kindly assist me with the above findings
Hello Jan!
I have visited my family doctor with my MRI results and he was unable to provide any clarification on how to read the results. I am hoping to post it here and get a better understanding and also some what I can do to improve the condition.
Procedure: Sagittal T1 and T2 and Axiai T2 through lumbar spine
There at 5 lumber type verebrae. The patient has developmentally short pedicales throughout the lumbar spine. The cord ends at L1-L2. No distal cord pathology.
L1-2: Mild disc bulge with borderline spinal stenosis. AP thecal sac a minimum dimension of 10mm. No exiting nerve root compression.
L2-3: Minimal disc bulge. Schmorl’s nodes. Mild facet degenerative changes. No Spinal Stenosis or exiting nerve root compression.
L3-4: Diffuse disc bulge with Schorl’s nodes. Mild facet degenerative changes. Borderline Spinal Stenosis with AP thecal Sac a minimum dimension of 10 mm. Borderline encroachment on both exiting L3 nerve roots.
L4-5: Minimla disc bulge. Early Schmorl’s nodes. Mild facet degenerative changes. No spinal stenosis or exiting nerve root compression.
L5-S1: Minimal disc bulge. Early Schmorls node into s1. Mild facet degenerative changes. No spinal Stenosis or exiting nerve root compression.
S1 nerver roots exit without compression.
Opinion: Developmentally short pedicles lead to boderline spinal stenosis ecen with mild hypertrophic degenerative changes. At worst, only borderline encroachment on exiting nerve roots and borderline spinal stenosis at L3-4. Multilevel early disc degenerative changed with Schmorl’s nodes in this young paitent.
T6-7 small Central protrusion effacing the ventral sac. There is mild canal stenosis.
T7-8 there’s a small left paracentral protrusion effacing the ventral thecal Sac with mild left foraminal narrowing
T8-9 there’s a small Central protrusion effacing the ventral thecal Sac with mild canal stenosis
T9-10 there is a small left paracentral protrusion effacing the ventral thecal Sac with mild left foraminal narrowing
T10-11 there’s a small Central protrusion effacing the ventral thecal Sac with mild canal stenosis
T11-12 there is a mild disc bulge
T12-L1 there is a right paracentral protrusion with annular fissure effacing the ventral thecal Sac resulting in moderate canal stenosis
Schmorl’s nodes seen along the inferior endplate of T10 11 and 12
Constant back pain hip pain radiating pain numbness and tingling chest pain radiating from the back also leg weakness and limping. I truly feel like my back is just going to snap and break this is been going on for years. Also are you familiar with the cervical spine at all. Thank you for any information you can give me I appreciate it. I was diagnosed with fibromyalgia for 10 years ago and often wonder if this is the culprit behind all of my symptoms also have balance issues
Looking through the Internet and found this site. I’m a 61-year-old male and I am completely flipping out. Sending this to you in hopes of any suggestions. I have read it 30 times and I still don’t know what I’m reading.
thank you
4/14/2018
David
Findings:
Intradural Space: The lower spinal cord and conus appear normal with no intradural masses or abnormalities
noted.
Osseous Structures and Bone Marrow: No compression fractures or deformities are identified. The marrow signal intensity is unremarkable.
Lower Thoracic Spine: No disc extrusions, herniations, or significant stenosis is noted of the visualized lower
thoracic discs.
Intervertebral Discs and Motion Segments:
L1-2: There is disc desiccation with a diffuse bulge causing mild impingement of the thecal sac. The foramina are mildly stenotic bilaterally when combined with facet hypertrophy.
L2-3: There is a diffuse disc bulge with eccentric component to the left. There is mild canal stenosis and left-sided foraminal stenosis when combined with facet hypertrophy and ligamentum thickening.
L3-4: There is a diffuse disc bulge with superimposed disc protrusion eccentric to the right causing moderate
foraminal stenosis and impingement of the right L3 root. Mild central canal stenosis is also noted best seen on
image 14 of series 5.
L4-5: There is a circumferential disc bulge with bilateral facet hypertrophy and ligamentum flavum thickening
resulting in mild impingement of the thecal sac and mild to moderate bilateral foraminal narrowing.
L5-S1: There is bilateral facet hypertrophy and a diffuse disc bulge causing impingement of the thecal sac without stenosis.
Visualized Sacrum:
The visualized sacrum is unremarkable. No abnormalities are identified of the sacral canal.
Paraspinal Soft Tissues:
Probable tiny renal cortical cysts are noted bilaterally. There is no evidence of solid
appearing paraspinal soft tissue mass.
IMPRESSION:
1. Multilevel disc bulges are seen throughout the lumbar spine causing impingement of the thecal sac. The disc bulge at L2-3 is eccentric to the left contributing to left-sided foraminal stenosis and canal stenosis.
2. At L3-4 in addition to disc bulge, there is a superimposed eccentric right lateral noncalcified 4mm protrusion causing moderate foraminal stenosis and impingement of the right L3 root. There is also mild central canal stenosis.
3. At L4-5 there is bilateral foraminal stenosis and impingement of the thecal sac secondary to diffuse disc bulge and facet hypertrophy.
25 year old female.
L4-L5 broad base disc bulge and legimentum flavum hypertrophy minimal central canal narrowing and minimal neural foranimal narrowing.
L5 s1 left foraminal disc protrusion approaching the exiting l5 nerve root minimal left neural foranimal narrowing
The conus terminates at L1
Can you please help me define what this means? Also would this be why I have a incredible amount of lower back pain and feet go tingly arms and hands do easily also have pain in my knees and legs… also have si joint problems!!!! Should I do injections like they recommend? I need help!!!!! Thanks
hii
i am critical care nurse which means i do lot of pushing and pulling big heavy patients. recently started having pain in lower back. my mri result
1. straightening
2. disc signal loss l, diffuse annular disc bulge L3-L4, L4-L5 deforming the thecal sac/ L4, L5 nerve roots
3. disc height reduction, spondylosis, facet joint hypertrophy impinging upon the left and right lateral neural foramina and exiting left nrlerve root, L5-s1
my doctor just i dont have worry much ” u worry too much” was his words. but i am worried and with kind of work i do i dont wanna worsen my condition. i also have some arthritic sympotoms in my knee making clicking sounds. i wondering if it means my bones r generaly weak causing this disc problem or is it not related. my vit d is also low. does taking calcium will help disc problems?? does the bulging heal by itself if i take rest. i have pain in back n leg but its not so bad. i am going see a pain mangement doctor too. should i consider changing to another unit?? pls suggest
Hello Jan, I hope you can help me know why I been in pain for 10 years. I had to stop working 2 years ago, pain was to much.
MRI says: There is normal alignment of the lumbar spine. Bone marrow signal is normal. Normal vertebral body height. The conus medullaris is at L1-L2 No significant narrowing of the spinal canal or foramina. L2-L3 No significant narrowing of the spinal canal or foramina. L3-L4 Diffuse disc bulge. Mild bilateral facet arthropathy. Mild bilateral neural foraminal stenosis. Mild spinal canal stenosis. L4-L5 Central posterior disc protrusion with annular fissure. Mild bilateral facet hypertrophy . Moderate bilateral neural foraminal stenosis. Mild spinal canal stenosis.. L5-S1 Diffuse disc bulge. Mild bilateral facet arthrophathy. Moderate to severe Right neural foraminal stenosis. Moderate Left neural foraminal stenosis. No significant spinal canal stenosis. Epidural lipomatosis is present at the L5 and S1 level with mass effect on the thecal sac. There is complete effacement of the CSF from around the nerve roots. Sacrum: Normal bone marrow signal.
The reports says you have diffuse disc bulges at L3-L4 and L5-S1 discs and a herniated disc with the fissure (crack) in the L4-L5 disc. L4-L5 disc , and to a lower extent, the other 2 discs are pressing upon the nerves. So, it is this compression of the nerves that can cause pain in the leg, and it is the crack in the disc which can cause the pain in the lower back. Additionally, there is some fat accumulation (lipomatosis) in the spinal canal (in which the spinal cord lies), possibly contributing to the symptoms. I don’t know where is this fat from. If the long-term rest does not help, you can discuss with your doctor about surgery.
Sir..My MRI LS SPINE REPORT SAYS…DISC DESICCATION WITH MILD DIFFUSE DISC BULGE NOTED AT LEVEL L5-S1 OF BILATERAL FJH(RIGHT>LEFT)…..DISC DESICCATION WITH DIFFUSE DISC BULGE AT LEVEL L4-L5 BILATERAL SEVERE NEURAL FORAMINA NARROWING AND LATERAL RECESS STENOSIS CAUSING NERVE ROOT COMPRESSION….AT L3-L4 LEVEL MILD LATERAL RECESS STENOSIS NEURAL FORAMINA NARROWING BILATERAL MILD LIGAMENTUM FLAVUM HYPERTROPHY……SIR PLEASE GUIDE ME..MY JOB IS PROLONGED SITTING…I M VERY DEPRESSED….PLZ HELP ME…
The reports says you have several bulging discs in the lumbar spine. Such discs may heal on their own with time (few months), but prolonged sitting is not optimal for that. You may want to get off the job for some time. You can also discuss with a doctor about surgery.
Sir..Is surgery is only option in my case.?? Can it be cure by physio or medicine or any other advice…I will follow each n every instruction of you sir… Kindly advise me..I shall be very thankful..I don’t want to go for surgery Sir…Plz guide me sir..You are only hope for people like me who are suffering from the same..Thnx a lot.
Sir..I forgot to tell you about my problem..I m suffering from extreme burning from my left hip to thigh area and pain in left hip.and burning has started in left side of back also..I m unable to sit… Please guide me with your extremely valuable advice..
Burning in the hip and pain in the back and leg can be all caused by pinched nerves due to bulging discs.
I’m not saying surgery is the only option, but if nothing other helps, on the end, it can help. If you have a sitting job and you are not able to sit, then I strongly suggest you to discuss with your doctor to approve sick leave. Then it is recommended to stay active, in the sense of being in “active rest” – moving around, changing positions, walking, concentrating on some activity and relationships rather on pain, but avoiding any physical work, lifting objects and bending. By doing only this, the bulging discs can heal on their own without any physiotherapy or drugs. It may take several months for this to work, not only one month.
As mentioned before, if the pain is unbearable, you can ask for analgesics or a steroid injection, but I’m not aware of any other drugs or herbal remedies that would cure the bulging discs. You may also want to find a good physiotherapist you can trust to show you some light stretching exercises – this needs to be discussed face to face, so I can’t recommend anything specific here.
At T11-T12 seen on sagittal images only, there is a broad-based central disc
protrusion that leads to mild canal stenosis.
L3-L4: There is a broad-based central disc protrusion
L2-L3: There is a diffuse disc bulge
What does this mean
Also what is suggestion for symptoms of lower back pain radiating down the right leg with leg weakness in ordinance of those findings ?
Thanks
It means, you have 3 bulging or herniated discs on the mentioned levels (in the lower thoracic and in the lumbar spine). The report does not say if there are any nerves pinched but the spinal canal (through which the spinal cord runs) is mildly narrowed – which may or may not cause any symptoms (in the legs?)
Thanks jan being kind and helpful. I will stick to your advise. So nice of you
Thanks jan for so much co-operation. I am asking so much questions but i am worried about this situation. I have rested for 1 month and but issue remains. What do you suggest on this issue?
By rest that can help to heal the discs it is usually meant avoiding lifting heavy objects and any heavier physical work in general, bending, prolonged sitting and driving. Rest here does not mean lying in bed or sitting all day. Walking can help relieve pain but other exercises may not help and may be harmful. Try to live as normally as possible. It may take few months for the pain to resolve and then additional few months for the discs to heal. You may want to read the article about a herniated disc.
I have an issue as i have back pain for last two months. MRI report says:
At L5/S1, minimal diffuse disc bulge and tiny annular tears in lateral recesses.
Minimal lateral recess/neuroforaminol stenoses seen . I am 26 year old. What are the complications in this situation? Whether special care is necessary?
Please help me in this situation. I am very worried
There is a minimal bulge and tear in the disc between the 5th lumbar and 1st sacral vertebra. This is what likely causes pain in the lower back.
The report says that the discs narrows the opening between the vertebra through which the root of the spinal nerve leaves the spinal cord, but it does not say if the nerve is pinched or not. If the nerve were pinched, you would likely have pain in the leg.
Such disc damage can be caused by an injury or can be a part of degenerative disc disease which can occur in individuals as young as you are. The damage described in the report can heal on its own with relative rest.
MRI report says…. There is a slight disiccation and moderate annular bulging at L4/L5 with impingement of the anterior thecal sac and L5 transiting nerve root…. there is a prominent annular fissure at L4/L5…. I have very bad lower back pain when doing simple tasks like vacuuming or washing up or standing in same position also numb right ankle and shin
The disc L4/L5 is degenerated (desiccated) and there is a crack (fissure) in it. This very likely explains the pain in the lower back. I strongly suggest you to avoid lifting anything heavy, repetitive bending and prolonged sitting or driving until the pain resolves. Numb ankle and shin are likely due to a pinched nerve (L5) caused by the degenerated disc.
Technique: Sagittal and axial T1WI, sagittal and axial T2WI, sagittal STIR images were taken through the lumbosacral spine. First degree retrolisthesis of L2 over L3 and L3 over L4. The vertebral body heights are preserved. No sign of vertebral body collapse. L2-L3 disk is desiccated, it shows central disk herniation indenting the anterior aspect of the thecal sac. No neural foramina compromise seen. L3-L4 disk is desiccated, it shows annular tear with central disk herniation indenting the anterior aspect of the thecal sac. No neural foraminal compromise seen. L4-L5 disk is desiccated, it shows annular tear with central disk protrusion. No neural foraminal compromise seen. L5-S1 disk is desiccated, it shows diffuse disk bulge indenting the anterior aspect of the thecal sac and compromises both lateral recesses. Normal dimensions of the spinal canal with no evidence of primary spinal canal stenosis. Normal MRI appearance of the conus medullaris and cauda equina. Cord ends opposite the L1. Normal marrow signal intensity of the scanned vertebrae. No remarkable paravertebral soft tissue abnormality. Opinion: First-degree retrolisthesis of L2 vertebra over L3 and L3 over L4. Multilevel degenerative disk changes most pronounced at the L5-S1.
The report says there are several degenerated (desiccated) discs in the lumbar spine but it appears they are not pressing upon the spinal nerves.
Many thanks Jan, so overall, is it a serious issue here or with some stretching exercises that might help to get back to normal. meanwhile, do you think to try to crack these areas which might help to get disks back?
The discs between the vertebra are made of cartilage and, in the center, of a soft substance that can bulge or herniate out due to repeated pressure. According to the report, there is a tear in the discs L3-L4 and L4-L5. The tears, bulging and herniation can heal on their own with time. You can read in this article about herniated disc that often the best therapy is rest and not exercise, “cracking” the area or physical therapy. By rest, I mean relative rest with avoiding lifting heavy objects, heavy physical work, bending, prolonged sitting or driving…not bed rest. Doctors usually encourage walking, though.
Early degenerative disc diseases with mild diffuse annular bulge noted at L4 – L5 level causing bilateral lateral recess and neural foraminal narrowing.
This report says that the disc between the 4th and 5th lumbar vertebra is bulged and that it narrows the openings through which the nerve roots go out of the spinal cord. The report does not say if the disc is pinching the nerves, but it could.
Thanks Jan for replay. Still have back ache and some its radiate to legs. Its heal on its own (within months) without any treatment.
Thanks for your replay. This disc bulge heal their own? Need any other medication or physio ? How long take to heal ?
Yes, such mild damage can heal on its own without any drugs, physiotherapy or surgery. It may take few months to heal completely. Try to avoid lifting anything heavy, any physical work, sports and prolonged sitting or driving. I’m not aware of any helpful exercises but walking is usually encouraged for this problem.
thanks for your reply. i just write here my MRI full report. please review.
lumbar lordosis maintained.
early degenerative disc diseases in the form of dehydration and loss of disc height noted at multiple levels.
mild diffuse annular bulge noted at L4-L5 level causing bilateral lateral recess and neural foraminal narrowing.
rest of vertibral bodies, pedicles, laminae, spinous and transverse processes show normal MR morphology, alignment and signal pattern. The bony spinal canal appears normal at each level.
the pre and para spinal regions do not showany demonstrable pathology.
the facet joints appear normal.
the conus medullaris and roots of cauda equina are normal in size, shape and signal pattern.
impression: Early degenerative disc diseases with mild diffuse annular bulge noted at L4 – L5 level causing bilateral lateral recess and neural foraminal narrowing.
now 4 weeks still have back pain like pin needle pain some times lower leg pain. i am afraid about it. its need more treatment? or rest ? now iam back in office. my job is sitting. its increase this condition? bulging? waiting for your reply. if need more rest i want to resign my job because i didn’t sick leave.
According to the symptoms, the disc L4/L5 is probably pinching the nerves that supply the legs. In general, the optimal treatment for such disc is rest: not rest in bed or constant sitting, but avoiding physical work, bending, carrying heavy objects and prolonged sitting or driving. Ideally, one could try frequently change his position: some walking, some sitting, some standing, and sleeping at night. Walking, for example at least 20 minutes once or few times a day, is the only exercise I believe it may help. I’m not sure if any physiotherapy or special exercises would help more than that. Painkillers by mouth or a steroid injection can help relieve the pain but you need to discuss this with a doctor.
Sitting as such may not worsen the condition but prolonged sitting could. So, if possible, you can try to interrupt the sitting by having some 20 minute walking.
MRI says,
-Central disk bulge at Level l2/l3 with moderate encroachment on the thesal sac
-Small cental disk protrusion at level L5/S1 and there appears to be mild encroachment on the origin of S1 nerve roots
-If this correlates to patient dermatomal distribution of symptoms, this site is amenable to CT guided steroid injection
Kindly assist me with the above findings
The report says there is a mild disc protrusion (herniation) that possibly causes a compression of the S1 nerve root. The doctor then suggests a steroid injection, if these MRI findings correlate with your symptoms (which would be sciatic pain down the leg).
Thanks for the response Jan. Will this disk herniation heal with out surgery. I am only 32 years old and bit worried with the risks involved with surgery.
The report says that the disc protrusion is small and the compression of the nerve is mild, which means there is a good chance the disc will heal on its own. I strongly suggest you to avoid anything what could worsen the disc protrusion, especially lifting heavy things and, if possible, prolonged sitting or driving.
Was wondering what my my MRI means and the severity of it. It reads as the followIMG
Vertebrae: Focus of T1 and T2 hyperintense signal in the posterior L3 vertebral body consistent with a hemangioma. Fatty endplate marrow signal changes posteriorly at L2-3 secondary to underlying degenerative disc disease. No Loss of vertebral body height.
Axial interbody analysis:
L1-L2: loss of disc height and signal consistent with disc desiccation No central canal or neural foraminal stenosis.
L2-L3: Marked loss of disc height and signal consistent with disc desiccation. Mild diffuse disc bulge resulting in minimal encroachment of bilateral neural foramen. There is mild flattening of the anterior thecal sac without significant central canal stenosis.
L3-L4: Mild diffuse disc bulge and facet arthropathy. No central canal stenosis. There is mild right and mild-to-moderate left neural foraminal stenosis.
L4-L5: Diffuse disc bulge with a small central disc protrusion. There is buckling of the ligamentum flavum and minimal facet arthropathy. No central canal stenosis. There is mild-to-moderate bilateral neural foraminal stenosis.
A hemangioma in L3 is a benign tumor in the third lumbar vertebra. Such tumor is not cancer (it does not spread) but may cause a local damage. A doctor may suggest further investigations to confirm diagnosis and tell the optimal treatment, which may involve a removal of the vertebra.
The other part of the report mentions various features of degenerative disc disease:
– “Disc desiccation,” = drying of the discs between the vertebra
– “Facet arthropathy,” = changes in the small articles between the vertebra
– Some “stenosis” (narrowing due to bulging disc), which may result in pinched nerves between the vertebra L2-L3, L3-L4 and L4-L5 (so this may be the most likely cause of eventual pain)
– “Diffuse disc bulge” = disc bulge that affects a large part of the disc circumference but is milder than disc herniation
– “Disc protrusion” = disc herniation
So, apart from hemangioma, there are changes in 4 lumbar discs that may or may not be responsible for symptoms. These changes do not seem to be very severe and may heal on their own but a doctor can suggest to fix them during eventual surgery for a hemangioma.
Hello Jan
My MRI states that:
L5-S1: there is a diffuse disc bulge with mild broad based left paracentral protrusion likely causing mild left lateral recess stenosis and mild right neuraforaminal stenosis.
Can you please suggestion some treatment options for this case ?
Is protrusion a herniation or disc bulge ?
Can we do spinal decompression (traction) for this type of problem ?
How much time does it take to heal a protrusion ?
I am sorry for asking too many questions but I am actively looking for opinions.
Thanks
Varsha
In this case, protrusion means herniation, because the report says it likely causes right neural foraminal stenosis, which means narrowing of the opening in the bone through which the nerve exits the spinal cord. It is said that the stenosis is mild, so it is quite possible it will heal on its own in a reasonable time – in weeks to few months. Try to avoid physical work, especially bending or lifting anything heavier than few kg, and also prolonged sitting or driving. Walking is fine.
It sounds possible that traction would provide some temporary symptoms relief but it may not shorten the healing time. It is a neurologist who can tell if there is any reason for any specific treatment.
At L4-L5 level disc desiccation
Diffuse circumferential disc bulge causing spinal canal and bilateral neural foraminal stenosis and compressing adjacent traversing and bilateral exiting nerve roots. Ligamentum flavum hypertrophy is seen adding to secondary canal stenosis
The disc between the vertebra 4 and 5 bulges out and presses upon the nerves that exit the spine on both sides. This may cause pain in the legs. It is an orthopedist or neurologist who can say what can be the optimal treatment.
Age -39 years
Male
MRI findings>
Opinion :Small posterocentral protrusion L4-5 disc
Diffuse disc bulge and a small left foraminal / extraforaminal posterior protrusion L5-S1 disc
Straightening of usual lumbar lordosis.The L-4-5 & L5-S1 discs are dessicated
L4-5 disc shows a posterocentral protrusion that indents the ventral theca
The L5-S1 disc shows a diffuse annular bulge and a small left foraminal/extraforaminal posterior protrusion that narrows the left l-5-s1 neural foramen
visualised vertebrae shows normal height and marrow signal.No antero or posterolisthesis seen. The lower cord and conus are unremarkable. No pre or paravertebral collection seen.The facetal joints are unremarkable .
problem faced by me is pain in lower back even while sitting and pain in legs and don’t feel comfortable in standing for longer durations. Job is getting affected as i am an engineer and need to lie down and access equipments at various odd/awkward postures and face difficulty in climbing stairs to reach at higher places.Already decided to switch job to one that requires less of physical fatigue and preferably to a office job.How good Is success rate of surgery? Can injections help in my case to cure ? or exercise? pl help in making me understand from any prospect?
The MRI report says there’s a protrusion of the discs between the L4 and L5, and L5 and S1 vertebra. Protrusion means herniation; you can read more here. Your symptoms sound like sciatica and are typical for this type of disc damage. Such herniation can often heal on its own (within months) without any treatment. An injection could temporary reduce lower back, but possibly not the leg pain. Surgery is quite effective but you may want to give the discs time to heal on their own.
The main thing you can do on your own is to prevent further disc damage by avoiding:
– lifting or carrying anything heavy (>5 kg) in the hands or carrying a heavy backpack
– prolonged sitting or driving or standing
– bending the back
– quick moves, climbing ladders, sports and such
Walking (>15 min) can reduce pain. Occasional changing position from standing to sitting can also help.
Predominantly sitting (office) job is NOT an ideal job for a herniated disc.
Thx doctor ! ? Will try to follow all mentioned preventions as advised to avoid any further damage to discs.
I’m not a doctor.
MRI SPINE LUMBAR WO CONTRAST – DetailsPrinter friendly page–New window will open
About This Test
Details
Study Result
Impression
IMPRESSION:
Lumbar spine degenerative changes are predominated by facet arthropathy at L4-L5 and mild bulging of the discs at L3-L4 and L4-L5.
Lumbar spine degenerative findings are as fully detailed above, without evidence of significant canal stenosis or exiting nerve root compression at any level.
VOICE DICTATED BY: Dr. Stetson Bickley
Narrative
EXAMINATION: MRI LUMBAR SPINE 9/1/2017 2:45 PM
ACCESSION NUMBER: 113280922
INDICATION: MRI Lumbar eval radiculopathy Pain across the lower back goes into left hip
COMPARISON: Lumbar spine x-rays 7/26/2017 lumbar spine MRI 10/1/2010
TECHNIQUE: Multisequence, multiplanar MR images were obtained of the lumbar spine without the administration of intravenous contrast.
FINDINGS: There are 5 lumbar vertebral bodies with vertebral body numbering performed with the designation of the last well formed intervertebral disc as L5-S1.
Vertebral body heights are preserved. Chronic type degenerative endplate changes of the anterior superior corner of L3 L3, anterior superior corner of L4, and anterior superior corner of L5. Probable lipid poor hemangioma at L3.
Level specific findings:
T12-L1: No significant canal or foraminal stenosis.
L1-L2: No significant degenerative change, neuroforaminal narrowing, or spinal canal stenosis.
L2-L3: No significant degenerative change, neuroforaminal narrowing, or spinal canal stenosis.
L3-L4: Minimal disc bulge. No significant canal or foraminal stenosis.
L4-L5: Mild bilateral facet arthropathy. Circumferential disc bulge. No significant canal or foraminal stenosis.
L5-S1: No significant degenerative change, neuroforaminal narrowing, or spinal canal stenosis.
The visualized portions of the distal spinal cord are of normal caliber and signal characteristics.. The conus medullaris terminates at the L1 level. The cauda equina is unremarkable.
Left renal cortical T2 hyperintensity is incompletely characterized but is probably a cyst.
What does all this mean. I am having terrible pain in my lower back.
In short: there is no pinched nerves and only two discs are mildly bulged. There are some changes in “facet joints,” which are joints on each side of the vertebra that connect vertebra with each other.
So, your pain might be due to “facet arthropathy,” which usually results from “wear and tear” of the spine.
You also seem to have a cyst in your left kidney.
Thank you.?
Straightning of lumber spine.
Disc decsiccation at L5 S1 level.
Mild disk bulge at L4 L5 level indicating thetical sac.
Diffuse disc bulged at L5 S1
These descriptions say that two discs (L4-L5 and L5-S1) are bulging out, but it does not say that they would pinch any nerve, so it is not sure if they cause pain.